
Anatomy of the knee joint
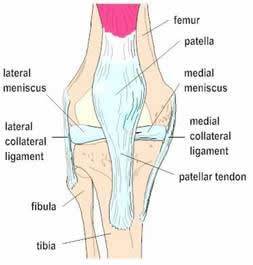
The knee is a hinge-type joint between the lower end of the femur (thigh bone) and the upper end of the tibia (shin bone). At the front of the knee is the patella (kneecap) which glides up and down in a groove in the lower femur when the knee bends and straightens. The quadriceps muscles are attached to the patella and these are responsible for straightening the leg. The patella is attached to the front of the tibia by the patellar tendon. There is also a thinner bone alongside the tibia called the fibula but this does not form part of the knee joint itself.


Antero-posterior and lateral x-rays of a knee outlining the bony anatomy
The knee is a complex joint and there are a number of important anatomical structures that support and stabilise the joint. These include muscles, ligaments and the menisci.
Muscles
The muscles of the thigh or quadriceps femoris muscles (quads) are critical to optimum knee function. When they contract the knee is straightened or extended by pulling on the kneecap. These muscles also have an important role in stabilising the knee. For this reason it is essential that the thigh muscles are as strong and effective as possible both before and after any major knee surgery. Careful and targeted physiotherapy restores muscle function and hence is a vital part of the overall treatment for any knee injury. If physiotherapy is not carried out then the full benefit of any reconstructive surgery may not become evident. The intensive six month rehabilitation programme following anterior cruciate ligament reconstruction best exemplifies this point. Strengthening muscles around the knee optimises the range of knee motion and decreases post-operative swelling.
Ligaments
Ligaments are bundles of strong fibrous material whose main role is to support and stabilise joints – they usually connect the two bones that make up the joint. There are two main sets of ligaments in the knee
- Collateral ligaments – the medial ligament is a broad flat band passing from the inside of the femur to the tibia and is about 10cm long and the lateral ligament is a rounded cord passing from the outside of the femur to the top of the fibula. These ligaments stop the knee from collapsing from side to side.
- Cruciate ligaments – the anterior cruciate ligament (ACL) lies within the knee joint, is about 4cm long and binds the tibia to the femur. The ACL prevents forward slipping of the tibia on the femur and stops hyperextension of the knee. The ACL is one of the most important stabilisers of the knee and when it is damaged patients often complain of giving way (please see below – knee injuries). The posterior cruciate ligament (PCL) lies just behind the ACL and similarly connects the femur and tibia but runs in a different direction. Its main role is to stop backward slipping of the tibia on the femur.
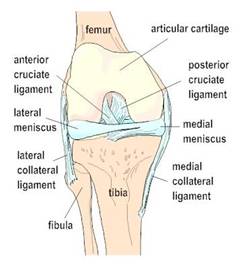
Anterior view of a right knee – in the lower image the
kneecap (patella) has been removed
Menisci
The menisci (plural of meniscus) are C-shaped shock absorbers that lie within the knee joint separating the femur from the tibia. There are two menisci in each knee – one on the inside (medial meniscus) and one on the outside (lateral meniscus). They are made of smooth white fibrocartilage and are triangular in cross section with the wider part sitting around the periphery of the knee joint and the thinner edge being more central. Apart from acting as shock absorbers the menisci contribute to joint lubrication and stabilisation. The upper surfaces are concave to receive the rounded ends of the femur. The under surfaces are flat and lie on the top of the tibia.
The medial meniscus is nearly semicircular in shape while the lateral meniscus is almost circular. The medial meniscus is more fixed than the more mobile lateral meniscus and for this reason is damaged more frequently in twisting injuries. Both menisci have a poor blood supply and hence when a meniscus is damaged or torn, complete healing is unlikely. A damaged meniscus is frequently referred to as a ‘torn cartilage’ and often requires arthroscopic surgery.
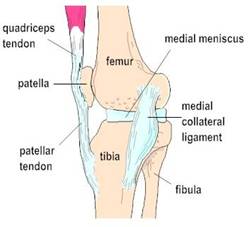
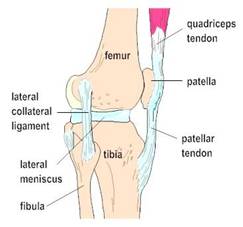
Medial (top) and lateral (bottom) images of a right knee
Osteoarthritis
Osteoarthritis is a name given to degenerative joint disease. This occurs when there is progressive breakdown of the joint surface or articular cartilage. Instead of the joint surfaces being smooth and essentially frictionless they become damaged and rough. Articular cartilage is a specialised shock absorbing material that unfortunately has very poor healing powers and once worn or damaged the changes become irreversible. The cartilage lining wears away and the knee is left with pain, reduced movement and stiffness. Weight-bearing joints in the lower limb (i.e. hip and knee joints) are subjected to significant load and are commonly affected. Deformity can occur in the knee and restriction of function is common.
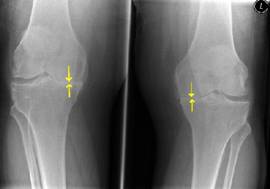
X-ray showing severe osteoarthritis (arrows) on the insides of
both knees leading to a bow-legged appearance
For younger patients there are some options with regard to surgery but ultimately a total knee replacement is often required to eliminate pain and restore movement. Osteoarthritis sometimes has no causative factors but obesity, previous injuries or surgery, joint instability, genetic or developmental abnormalities and metabolic diseases can contribute to the problem.
Rheumatoid Arthritis
Rheumatoid arthritis is a chronic inflammatory disease and can affect knee and hip joints. It is an auto-immune disease whereby cells in the body can turn on cells in the linings of joints causing pain, redness and swelling. The exact cause is poorly understood. Articular cartilage is damaged, ligaments become weak and surrounding bone can be destroyed. The ultimate result is a very worn out joint that often requires replacing. Even though rheumatoid arthritis is treated by rheumatologists and treatment can involve steroid injections and very effective modern day drugs, treatment frequently involves orthopaedic surgery.
Knee Injuries
The knee due to its complexity is a frequently injured joint especially amongst football and rugby players and athletes involved in impact activities. In addition a simple fall or a twist can cause problems that may require a surgical solution. Obviously fractures around the knee can occur and these frequently require internal fixation with plates and screws. Clearly this type of surgery is undertaken as a matter of utmost urgency. Mr Rees carries out such operations almost exclusively at Broomfield Hospital via the Accident & Emergency Department. Plain x-rays usually uncover a bony injury but CT (computer tomography) scans are also routinely used to give more accurate and detailed information about a possible fracture.
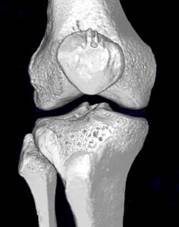
Three dimensional CT reconstruction of a knee joint
showing the bony outlines very clearly
However it is damage to the extensive soft tissues within the knee that can cause more subtle problems and these sometimes can be a little more difficult to immediately diagnose.
Frequently the knee swells up significantly due to bleeding, movement is restricted and weight bearing is painful or impossible. In these cases the plain x-rays may well be normal. However the menisci can be torn as mentioned above and cause problems of giving way and pain, the collateral ligaments can be stretched or torn causing pain and weakness on the sides of the knee and the cruciate ligaments can be ruptured causing instability between the femur and the tibia. In addition as a result of a nasty twisting injury of the knee the end of the thigh bone can also be forcibly squashed down on the top of the tibia causing damage to the normally smooth articular cartilage within the joint. Physiotherapy is a very important treatment modality for all knee injuries and sometimes this is all that is required. If symptoms persist then surgery is an option and recovery times will vary depending on the exact extent and nature of the injury.
In order to help outline which structures are damaged further imaging in the way of magnetic resonance imaging (MRI) is often required. This is a very safe way of gaining detailed information about the knee and takes about 20 minutes in a scanner. There are high quality MR scanners at the Chelmsford Medical Centre, the Capio Springfield Hospital and Broomfield Hospital.


