
The patella (kneecap) normally sits in a groove in the end of the femur (thighbone) called the trochlea. When the knee bends and straightens the patella moves up and down in this groove. This movement is termed ‘patellar tracking’ and if the patella sits centrally on the femur and does not deviate then no symptoms arise.
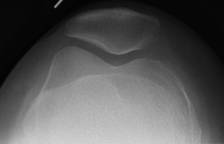
Skyline x-ray showing normal patella sitting
centrally in the trochlea of distal femur
However if the patella has excessive outward or lateral forces then it can move in an abnormal fashion causing discomfort and a feeling of instability. This is termed ‘patellar malalignment’. In severe situations the patella can even dislocate from its correct position and pop out of the side of the knee. Often this follows a serious injury but if ligaments around the patella are damaged then recurrent instability can result.

Skyline x-ray showing an abnormal tilted or subluxed patella
Usually the thigh muscles (especially the quads) can be strengthened and retrained to stabilise the patella with targeted physiotherapy. Occasionally a knee brace that centralises the kneecap can help alleviate anterior knee pain but if conservative options fail then surgery is sometimes required to restore overall patellar alignment. Patellofemoral pain and instability are difficult symptoms to treat successfully and unfortunately proceeding to surgery may not guarantee an end to the problems and patients must be aware of this possibility.
Nevertheless patella realignment surgery can be very effective and takes several forms. The most simple operation is an arthroscopic ‘lateral release’ whereby through keyhole surgery the tight lateral structures can be cut to allow the kneecap to sit more centrally. Sometimes this procedure is not enough and needs to be combined with a reinforcement or double breasting (reefing) of the weakened medial structures including some of the quadriceps muscles (VMO advancement).
There are further procedures which involve pulling the patella medially by releasing the lateral part of the patellar tendon and bringing it over medially and reattaching it onto the tibia. This is commonly performed in conjunction with a lateral release and a medial reefing. Occasionally there may be a requirement for the bony attachment of the patellar tendon to be physically moved more medially to help the patella sit more centrally in the trochlea. The bone is then re-fixed with two screws. Following this operation the patient is required to wear a brace for between 8-12 weeks depending on the rate of healing. This surgery can has fallen out of favour to a certain extent as it can lead to a painful prominence at the top of the shin bone and even overcorrection of the initial problem.
One procedure gaining popularity is reconstruction of the medial patellofemoral ligament (MPFL). When a kneecap fully dislocates laterally the chances are that the MPFL will have been ruptured or at best severely stretched and weakened. An MR scan can accurately diagnose such an injury. Similar to an ACL reconstruction, a length of hamstring tendon can be harvested from the lower thigh and can be used to bind the kneecap to the inside of the thigh bone thereby decreasing the likelihood of the kneecap being pulled outwards. As with every operation there are risks which include infection, blood clot, neurovascular damage, persisting pain and recurrent instability.
The treatment for patellar malalignment is not particularly straightforward but clearly physiotherapy is very important. There are several surgical options and Mr Rees would be happy to discuss the pros and cons of proceeding to surgery with patients who demonstrate patellar problems.