
Knee arthroscopy is a form of ‘keyhole’ surgery. It is an operation during which a small telescope called an ‘arthroscope’ is inserted into the knee. Attached to the arthroscope is a fibre optic cable which carries the image back to a monitor. At the same time small instruments can also be inserted into the knee in order to treat any problems encountered. Photographs of inside the knee are taken during the surgery to demonstrate to the patient what was found and what was carried out.
Arthroscopy is sometimes required to find out what is causing problems within the knee. It is however particularly recommended for the following knee conditions
- A meniscal tear (this can be repaired or smoothed away)
- Loose bodies (small pieces of bone or cartilage can be removed)
- Mild to moderate arthritis of the knee (the knee can be washed out)
- Inflamed lining of the knee joint (the synovium can be removed – this can benefit patients with rheumatoid arthritis)
- A damaged or ruptured cruciate ligament (this can be diagnosed and the frayed ends tidied up)
- Patellar maltracking (a lateral release can be performed to help the kneecap sit in a more comfortable position)
The surgery is carried out under general anaesthetic and usually as a day case – i.e. no overnight stay. Occasionally a spinal anaesthetic is given in preference to a general anaesthetic and this can be discussed with the anaesthetist beforehand. A tourniquet is placed around the upper thigh to allow a bloodless operative field. Two small ‘stab’ incisions or ‘portals’ are made either side of the patellar (kneecap) tendon. They are approximately 6mm in length.
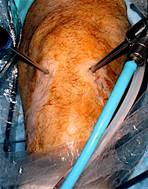

Peri-operative photos showing knee arthroscopy through keyhole incisions
One portal is for the arthroscope and the other is used for inserting small surgical instruments such as a blunt hook or probe, scissors, a punch and electric shaver. Saline (salt solution) is pumped into the knee joint to help stop any bleeding and to open up the joint to make the operation easier. Additional portals can also be used depending on the findings during the procedure in order to increase access to all parts of the knee. The whole operation usually lasts no more than 45 minutes.
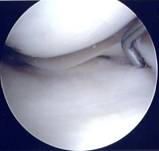
Arthroscopic photo showing a hook probing a normal medial meniscus

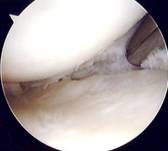
Arthroscopic photo showing a shaver smoothing a degenerate meniscus

Arthroscopic photo of loose body floating (piece of cartilage) in knee

Arthroscopic photos showing on the left a tear of the medial
meniscus and on the right a shaver debriding the tear


Arthroscopic photos showing loss of articular cartilage in a very arthritic knee
If one of the cruciate ligaments is found to be ruptured during an arthroscopy it will not be reconstructed at this time unless specifically discussed with the patient. Once a damaged cruciate ligament is diagnosed a lengthy period of physiotherapy is required prior to a definitive operation (ACL reconstruction) after which a typical recovery time is between 9 and 12 months.
At the completion of the surgery the knee is thoroughly washed out with saline solution (sometimes up to 6 litres) to clear the knee of any debris. All of the saline is drained and small sutures are used to close the portals in the skin. Local anaesthetic is injected into the knee to offer pain relief immediately after the operation. The knee is then bandaged up with wool and crepe and this stays in place for 48 hours. The sutures are removed 10 days after the surgery.
Patients stay in hospital for between 3 and 6 hours after the surgery. Full weight bearing is usually permitted (depending on the exact nature of the surgery) and crutches are issued to aid walking just for a few days. Simple pain medication is prescribed for a few days as the knee will ache after the surgery. Physiotherapy is then required to help strengthen muscles around the knee and this will be arranged prior to discharge. Patients are reviewed in the clinic after approximately 6 weeks to check on progress.
Patients should not drive for about 2 weeks after knee arthroscopy but more precise advice is given to individual patients. Most patients can return to work in about 7 days if the job involves mainly sitting. If a job is more manual or demanding sometimes a delay of between 2 and 3 weeks is advised. Participation in most sports including swimming should be possible after 3 weeks. However it must be recognised that full recovery can take many months.
Complications following knee arthroscopy are fortunately rare but can occasionally occur. These include infection, deep vein thrombosis, excessive swelling or bleeding and damage to blood vessels or nerves around the knee. In addition it is possible that in some patients the pre-operative symptoms do not significantly improve after arthroscopy.